
It's named after an octopus trap — and that's not all that's unusual about this reversible heart condition. It occurs almost exclusively in women.
Years of gender-based research have shown that in matters of the heart, sex differences abound. One striking example is the temporary heart condition known as takotsubo cardiomyopathy, first described in 1990 in Japan. More than 90% of reported cases are in women ages 58 to 75. Research suggests that at least 6% of women evaluated for a heart attack actually have this disorder, which has only recently been reported in the United States and may go largely unrecognized. Fortunately, most people recover rapidly with no long-term heart damage.



Features of takotsubo cardiomyopathy
|
What is it?
Takotsubo cardiomyopathy is a weakening of the left ventricle, the heart's main pumping chamber, usually as the result of severe emotional or physical stress, such as a sudden illness, the loss of a loved one, a serious accident, or a natural disaster such as an earthquake. (For additional examples, see "Stressors associated with takotsubo cardiomyopathy.") That's why the condition is also called stress-induced cardiomyopathy, or broken-heart syndrome. The main symptoms are chest pain and shortness of breath.
Stressors associated with takotsubo cardiomyopathy*
*Not an exhaustive list.
Sources: Prasad A, et al. American Heart Journal (2008), Vol. 155, No. 3, pp. 408–17; others.
|
�
The precise cause isn't known, but experts think that surging stress hormones (for example, adrenaline) essentially "stun" the heart, triggering changes in heart muscle cells or coronary blood vessels (or both) that prevent the left ventricle from contracting effectively. Researchers suspect that older women are more vulnerable because of reduced levels of estrogen after menopause. In studies with rats whose ovaries had been removed, the ones given estrogen while under stress had less left-ventricle dysfunction and higher levels of certain heart-protective substances.
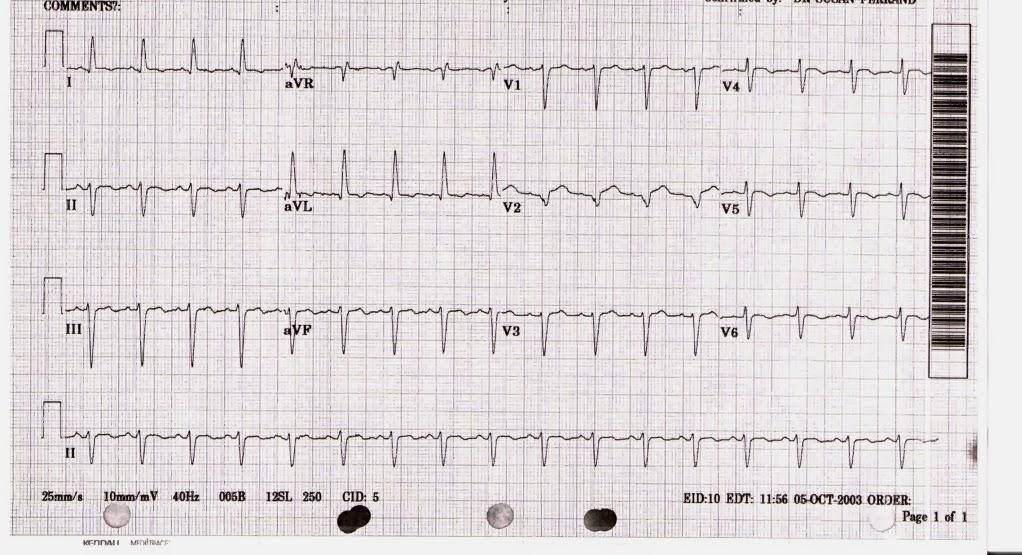
Takotsubo symptoms are indistinguishable from those of a heart attack. And an electrocardiogram (ECG) may show abnormalities also found in some heart attacks — in particular, changes known as ST-segment elevation. Consequently, imaging studies and other measures are needed to rule out a heart attack. To get a definitive diagnosis, clinicians look for the following:
- No evidence on an angiogram of blockages in the coronary arteries — the most common cause of heart attacks. (The coronary arteries are also not blocked in microvessel disease, a more common cause of heart attack symptoms in older women. Microvessel disease results from abnormal dilation of the blood vessels feeding the heart.)
- A rapid but small rise in cardiac biomarkers (substances released into the blood when the heart is damaged). In a heart attack, cardiac biomarkers take longer to rise but peak higher.
- Evidence from an x-ray, echocardiogram (ultrasound image), or other imaging technique that there are abnormal movements in the walls of the left ventricle. The most common abnormality in takotsubo cardiomyopathy — the one that gives the disorder its name — is ballooning of the lower part of the left ventricle (apex). During contraction (systole), this bulging ventricle resembles a tako-tsubo, a pot used by Japanese fishermen to trap octopuses. Another term for the disorder is apical ballooning syndrome. (See "Apical ballooning and the tako-tsubo.")
�
Apical ballooning and the tako-tsubo
An x-ray of the left ventricle (A) shows apical ballooning, a reversible abnormality characteristic of takotsubo cardiomyopathy. During systole (cardiac contraction) the midsection and tip (apex) of the left ventricle balloon out, while the area above, called the base, contracts normally. The shape is similar to that of a tako-tsubo (B), a round-bottomed, narrow-necked vessel used to catch octopuses.
Photos reprinted with permission from Bilal Saeed, M.D., University of Toledo Medical Center, Toledo, Ohio (A), and Satoshi Kurisu, M.D., Hiroshima City Hospital, Hiroshima, Japan (B).
|
�
Treatment
There are no evidence-based guidelines for treating takotsubo cardiomyopathy. Clinicians usually recommend standard heart failure medications such as beta blockers, ACE inhibitors, and diuretics (water pills). They may give aspirin to patients who also have atherosclerosis (plaque buildup in the arterial walls). Although there's little evidence on long-term therapy, beta blockers (or combined alpha and beta blockers) may be continued indefinitely to help prevent recurrence by reducing the effects of adrenaline and other stress hormones. It's also important to alleviate any physical or emotional stress that may have played a role in triggering the disorder.
Most of the abnormalities in systolic function and ventricle wall movement clear up in one to four weeks, and most patients recover fully within two months. Death is rare, but heart failure occurs in about 20% of patients. It's treated with diuretics, agents that improve heart muscle contraction, and other therapies. Rarely reported complications include arrhythmias (abnormal heart rhythms), obstruction of blood flow from the left ventricle, and rupture of the ventricle wall.

No comments:
Post a Comment